23/M with fever and backache
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
CASE:
A 23 year old man, resident of Nakrekal and goldsmith by occupation, has come to the OPD with chief complaints of fever and backache since 6 days.
History of Present Illness:
The patient was apparently asymptomatic 6 days ago, then he developed fever (high grade) which was continuous, not associated with chills and rigor. It got subsided on taking medication given by a local RMP.
He also complains of backache since 6 days which was insidious in onset, gradually progressive and continuous.
He also had an episode of vomiting today (1st Dec 2022) which was non projectile and had food particles in it.
He also complains of abdominal pain which is insidious in onset and not associated with nausea and vomiting.
He had an episode of passage of mild black coloured stools today (1st Dec 2022) which was soft in consistency and not associated with any blood, mucus or foul smell.
No history of loose stools, burning micturition, reduced urine output or difficulty in micturating.
Daily Routine:
He wakes up by 7 AM in the morning, does his morning routine and has his breakfast by 9 AM and off he goes to work by 10 AM (He’s a goldsmith). He usually has 3 Idlis or 2 Dosas for breakfast.
He has his lunch by 1 PM. He usually has rice and curry (mostly vegetarian).
At 4 PM, he has tea with biscuits.
Winds up his work by 8 PM and returns home.
He has his dinner by 9 PM. He has rice and curry. Occasionally he eats chapati (2)
He goes to bed by 11 PM in the night.
Past History:
History of fever, 6 days ago which was suspected to be Typhoid and was given medication for it.
No history of hypertension, diabetes, asthma, epilepsy and TB.
No history of previous surgeries.
Family History:
No history of similar complaints in the family.
Personal History:
Diet: Mixed
Appetite: Normal
Sleep: Adequate
Bowel and Bladder Movements: Regular
He consumes beer (1 or 2) occasionally.
Treatment History:
He was given DOLO 650 mg for 3 days.
General Examination:
Patient was conscious, coherent and cooperative. Moderately built and nourished. Well oriented to time, place and person.
Vitals -
Temperature - afebrile
BP - 110/80 mmHg
Pulse - 82 bpm
RR - 16 cpm
No pallor, icterus, clubbing, cyanosis, lymphadenopathy and oedema.



Systemic Examination:
CVS: S1 and S2 were heard. No murmurs.
RS: Normal bilateral vesicular breath sounds were heard.
CNS: No focal neurological deficit.
Abdomen: No abdominal tenderness and organomegaly.

Investigations:

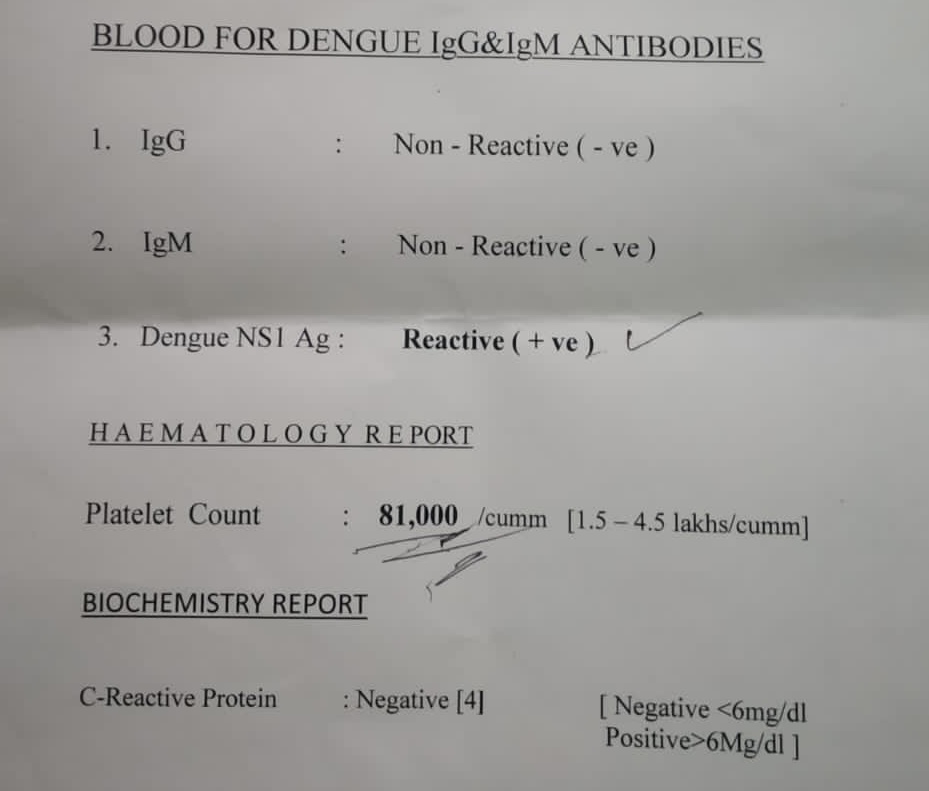
Provisional Diagnosis:
Dengue fever (NS1 positive)
Treatment:
IVF - NS/RL 500 ml IV
Inj Neomol IV/SUS ( if temperature is > 100 degree F)
Tablet Dolo 650 mg PO/BD
Inj Zofer 4mg IV/OD
Inj Pantop 40 mg IV/OD


Comments
Post a Comment