58/F with uncontrolled sugar and fever
This is online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs .This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome.



No Abdominal distension
No scars, sinuses, mass visible
Palpation:
Inspectory findings are confirmed
No local rise of temperature
Tenderness
Auscultation
Normal bowel sounds heard
RESPIRATORY SYSTEM EXAMINATION
Inspection:
Bilaterally Symmetrical chest movements present
No scars and sinuses
Trachea central
Palpation:
Inspectory findings are confirmed
Percussion:
Resonant note present in all lung areas
Auscultation:
Normal vesicular breath sounds heard.
Inspection : Bilaterally symmetrical chest present
No scars, sinuses
Palpation:
Inspectory findings are confirmed
Apex beat normal
On Auscultation :
S1 S2 heard, no murmurs or additional heart sounds
CENTRAL NERVOUS SYSTEM EXAMINATION
Higher mental functions intact
Cranial nerves intact
No focal neurological defecits
Provisional diagnosis
Viral pyrexia with uncontrolled sugars
Investigations
GRBS
14/8/2022
8am 254mg/dl
2pm 343mg/dl
8pm 337mg/dl
15/8/2022
8am 89mg/dl
2pm 147mg/dl
8pm 137mg/dl
16/8/2022
8am 197mg/dl
2pm 305mg/dl

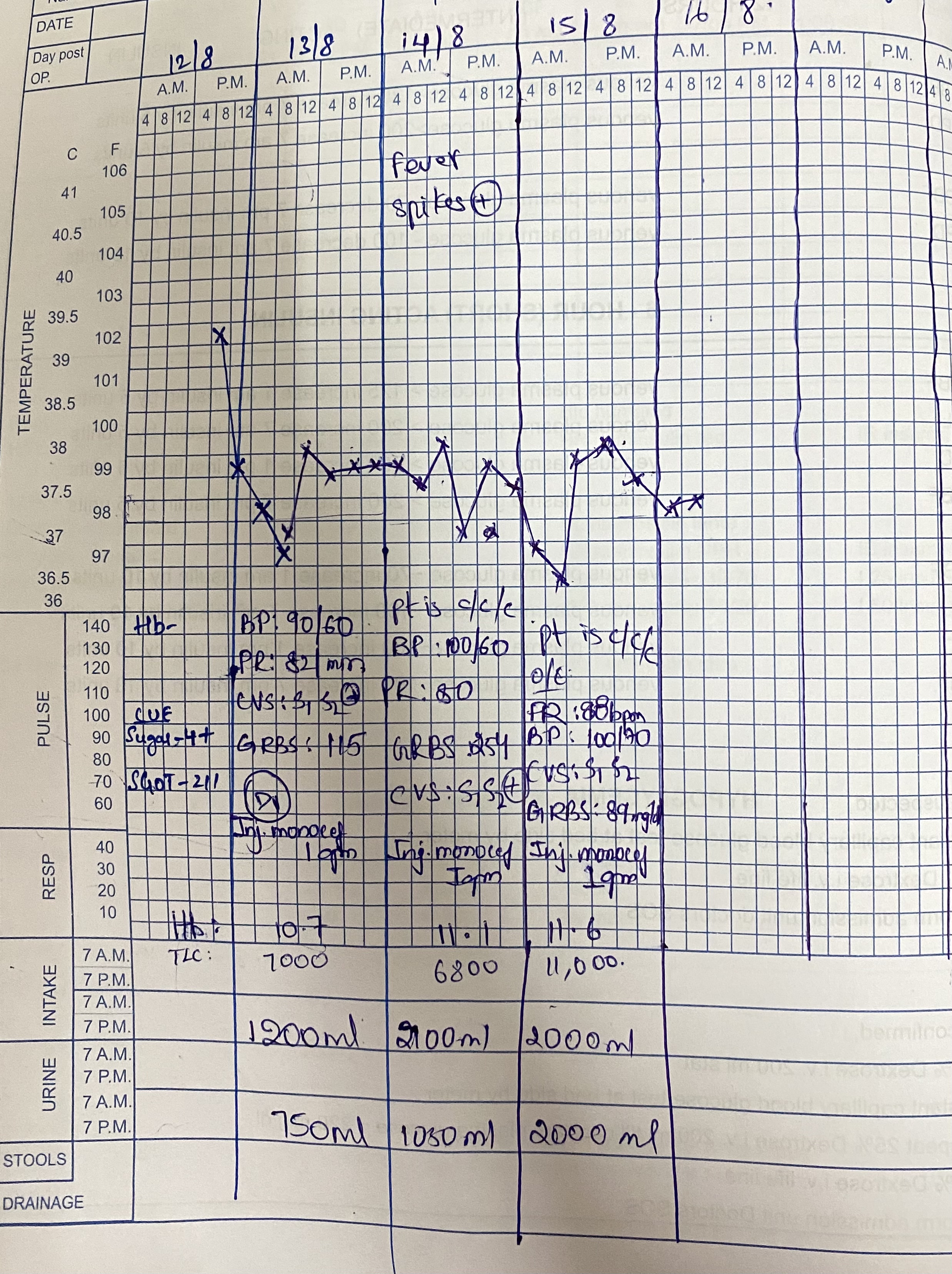




Treatment
IV fluids NS RL @50ml/hr
Inj.MONOCEF 1gm IV BD
Inj.PAN 40mg IV OD
Inj.NEOMOL 1gm IV(if required)
Inj. HAI 6-6-6units SC TID
Inj. NPH 10-8units SC BD
Tab. DOLO 650mg PO TID
Tab. DOXY 100mg PO BD


Comments
Post a Comment