40/F with high grade fever
This is online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs .This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome.
40 year old female with to casualty with complaints of
high grade fever since 5-6 days
C/o vomitings since yesterday
C/o loose stools since today.
History of presenting illness :
Patient was apparently asymptomatic 5-6 days then she developed fever , sudden high grade not a/w chills and rigors , intermittent, relieved temporarily on medication.
C/i vomiting since yesterday h/o 3-4 episodes , content good particles ,non bilious , non projectile , nausea present
C/o abdominal bloating since yesterday
C/o SOB since yesterday , releived on lying down,
No chestpain , palpitations PND orthopnea
C/o loose stools since today , watery consistency, 4-5 episodes ,small quantity, non blood stained , not associated with pain abdomen.
C/o epigastric pain since today , insidious onset , continuous , non radiating
Past history :
N/k/c/o HTN DM CVA CAD TB ATHMA
K/c/o Hypothyroidism since 10 years on tab. Thyronorm 100mcg /po/ od using irregularly since 15 days
Family history :
No similar complaints
Personal history :
Sleep : Normal
Diet : Mixed
Appetite : Normal
Bowel and Bladder Movements : Regular
Addictions : none
General examination :
Pt is c/c/c
No pallor , icterus , cyanosis, clubbing, lympadenopathy, edema
Vitals :
PR: 124bpm
RR: 18cpm
BP: 70 systolic ( palpatory)
GRBS : 183mg%
Systemic examination :
CVS : S1 s2 heard no murmurs
RS : BAE NVBS heard
P/A : epigastric tenderness present
No free fluid.
CNS : No FND




Investigations :







Ultrasound :


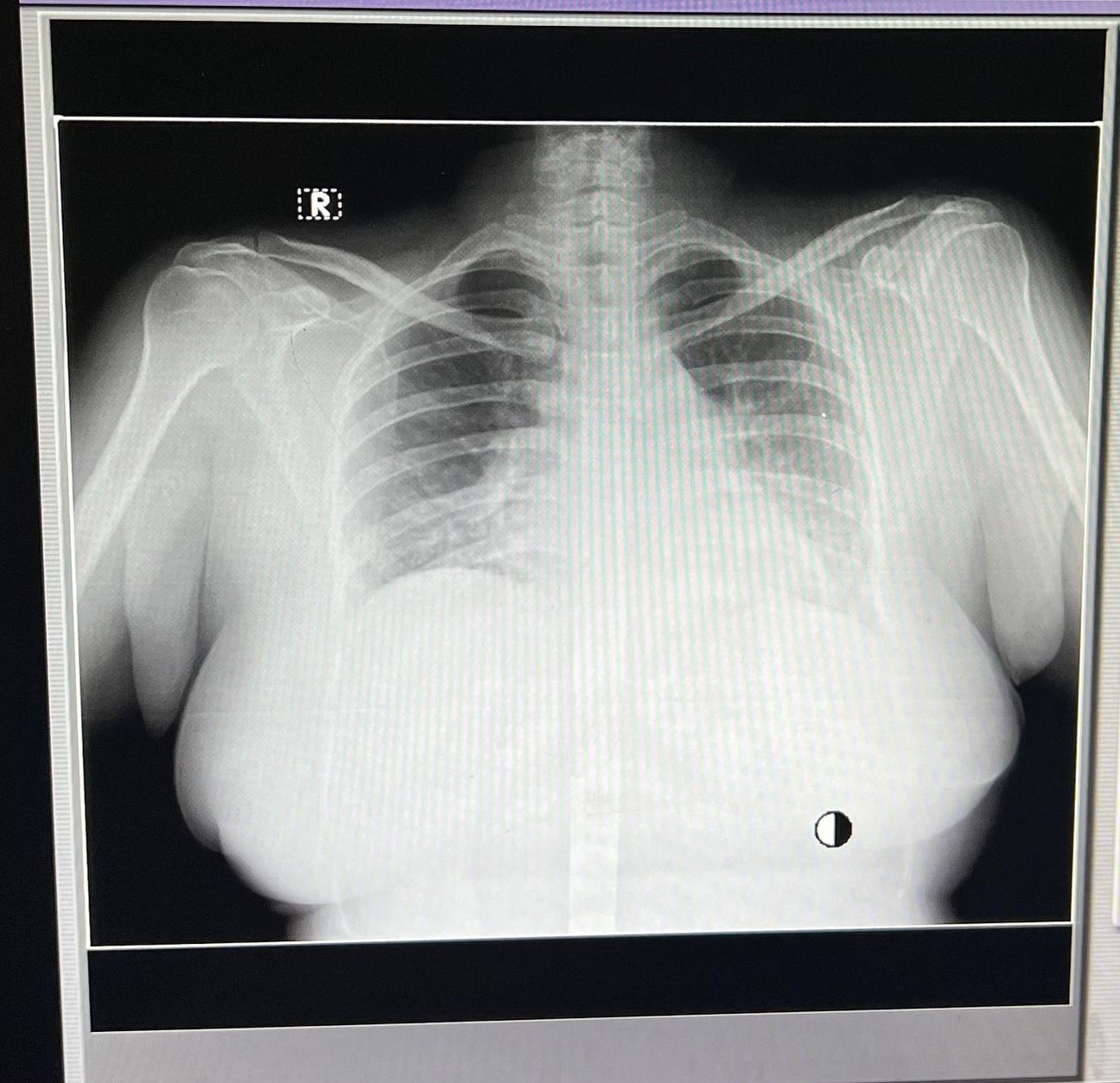
X-RAY CHEST :
Treatment :
IV FLUIDS NS & RL @100ML/HR
INJ.PIPTAZ (D6) 2.5GM IV /TID
(D5) TAB. AZITHROMYCIN 500MG PO/OD 8AM
T. THYRONORM 100MCG PO/OD
(8AM- 15MINS BEFORE FOOD)
INJ. DROTIN IM/SOS
INJ. PAN 40MG/IV/BD
INJ. ZOFER 4MG IV/BD
Fever chart :

Soap notes :
Soap notes
10/6/2023
AMC Cubicle
Dr. Zain (SR)
Dr. Pavan (PGY2)
Dr. Lohith (PGY1)
S:
- SOB resolving
- Pain abdomen resolving (hypochondrium)
- Did not pass stools
- No fever spikes
O:
Pt has conscious, coherent, cooperative.
BP: 110/70mmhg
PR: 82 bpm
RR: 16 cpm.
Spo2: 99%
CVS: S1 s2 heard , no murmurs RS: B/L air entry present NVBS +
Decreased air entry in lt. IMA
P/A: mild tenderness in right hypochondrium
A:
HYPOVOLEMIC SHOCK SEOCNDARY TO ACUTE GE (RESOLVED)
? COMMUNITY AQUIRED PNEUMONIA
WITH ? LEFT LOWER LOBE PNEUMONIA (BACTERUA US ATYPICAL)
WITH ACUTE CALCULUS CHOLECYSTITIS
WITH K/C/O HYPOTHYROIDISM
P:
IV FLUIDS NS & RL @100ML/HR
INJ.PIPTAZ (D6) 2.5GM IV /TID
(D5) TAB. AZITHROMYCIN 500MG PO/OD 8AM
T. THYRONORM 100MCG PO/OD
(8AM- 15MINS BEFORE FOOD)
INJ. DROTIN IM/SOS
INJ. PAN 40MG/IV/BD
INJ. ZOFER 4MG IV/BD
MONITOR VITALS 4TH HOURLY
Soap notes
11/6/2023
AMC Cubicle
Dr. Zain (SR)
Dr. Pavan (PGY2)
Dr. Lohith (PGY1)
S:
- SOB resolving
- Pain abdomen resolving (hypochondrium)
- Did not pass stools
- No fever spikes
O:
Pt has conscious, coherent, cooperative.
BP: 110/70mmhg
PR: 82 bpm
RR: 16 cpm.
Spo2: 99%
CVS: S1 s2 heard , no murmurs RS: B/L air entry present NVBS +
Decreased air entry in lt. IMA
P/A: mild tenderness in right hypochondrium
A:
HYPOVOLEMIC SHOCK SEOCNDARY TO ACUTE GE (RESOLVED)
? COMMUNITY AQUIRED PNEUMONIA
WITH ? LEFT LOWER LOBE PNEUMONIA (BACTERUA US ATYPICAL)
WITH ACUTE CALCULUS CHOLECYSTITIS
WITH K/C/O HYPOTHYROIDISM
P:
IV FLUIDS NS & RL @100ML/HR
INJ.PIPTAZ (D6) 2.5GM IV /TID
(D5) TAB. AZITHROMYCIN 500MG PO/OD 8AM
T. THYRONORM 100MCG PO/OD
(8AM- 15MINS BEFORE FOOD)
INJ. DROTIN IM/SOS
INJ. PAN 40MG/IV/BD
INJ. ZOFER 4MG IV/BD
MONITOR VITALS 4TH HOURLY


Comments
Post a Comment